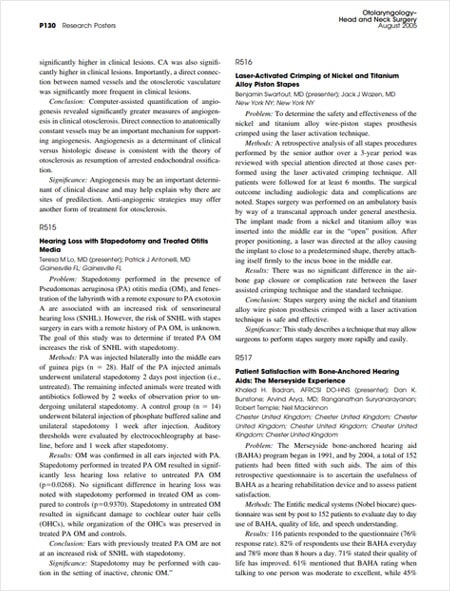
Benjamin G. Swartout, M.D. Facial Plastic Surgeon
Dr. Swartout is a California native who attended college at Harvard and went on to medical school at Albert Einstein College of Medicine in New York. He then did his internship in general surgery at New York University, followed by a specialty residency in Otolaryngology, Head & Neck Surgery at New York University. Following his specialty training, he completed a fellowship in Facial Plastic & Reconstructive Surgery at the University of Illinois at Chicago, where he worked with Dr. Dean Toriumi. The focus of the training in Chicago was on revision rhinoplasty and the use of rib cartilage grafts.
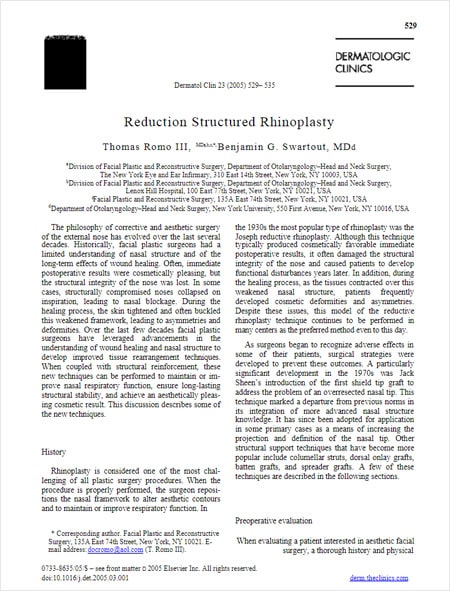
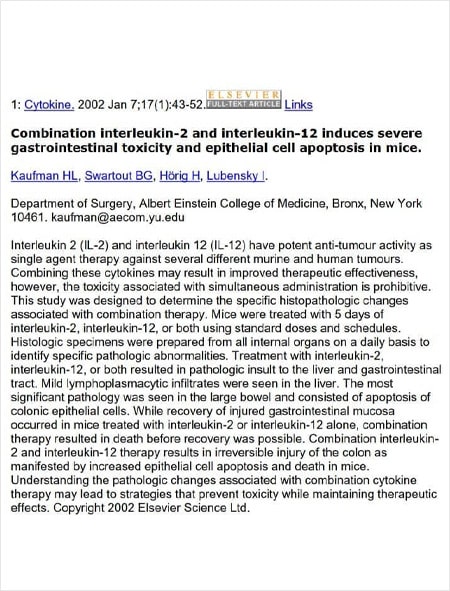
Dr. Swartout has published numerous articles and book chapters focusing on aesthetic facial surgery, specifically rhinoplasty, revision rhinoplasty, and ethnic rhinoplasty. In his practice, he sees many patients who have had prior rhinoplasty by other surgeons and now require correction. His special interests include the development of rhinoplasty techniques to create long-lasting, favorable nasal shapes and good nasal breathing. He teaches nasal surgery to residents at Harbor UCLA, both to contribute to the education of future doctors and to give back to an underserved community.
Dr. Swartout
Benjamin G. Swartout, M.D. is a fellowship-trained subspecialist in Facial Plastic surgery. He is passionate about providing high-quality care to his patients and creating natural, unoperated-looking results.
-

- Real Patient

Dr. Swartout Academy Memberships
- American Academy of Facial Plastic & Reconstructive Surgery
- American Academy of Otolaryngology, Head & Neck Surgery
- American Rhinologic Society
Awards
- Healthgrades Honor Roll
- Southern California’s Super Doctors 2020
Articles


Over 10 years of experience in Facial Plastic Surgery
4.8
22 ratings
Vitals
4.6
6 reviews
RateMDs
5
5 reviews
HealthGrades
Dr. Swartout Education
- College: Harvard, Cambridge, MA
- Medical school: Albert Einstein College of Medicine of Yeshiva University – 2001
- Internship in General Surgery: New York University Medical Center – Pathology Residency & Fellowship Programs – 2002
- Residency in Otolaryngology: New York University Medical Center – Pathology Residency & Fellowship Programs – 2006
- Fellowship in Facial Plastic & Reconstructive Surgery: Dean Toriumi at the University of Illinois, Chicago – 2007
The Dr. Swartout Approach
Dr. Swartout’s approach to facial plastic surgery, particularly rhinoplasty, is rooted in creating aesthetically pleasing and lasting results while ensuring optimal nasal function. He specializes in correcting surgeries previously performed by other surgeons, emphasizing revision rhinoplasty and ethnic rhinoplasty. His technique is patient-centered, focusing on the individual needs and aesthetic goals of each patient. Dr. Swartout’s commitment to his craft is evident in his dedication to teaching and sharing his expertise in nasal surgery with residents at Harbor UCLA, aiming to improve both the form and function of the nose with each procedure.
Benefits of a Facial Plastic Surgeon Consultation in Beverly Hills
Choosing Dr. Swartout for facial plastic surgery offers multiple benefits. Patients benefit from his extensive training and expertise, particularly in complex revision and ethnic rhinoplasty cases. His academic contributions to the field, including numerous published articles and book chapters, reflect his deep understanding of facial aesthetics and surgery techniques. Moreover, Dr. Swartout’s dedication to community service and education ensures that he remains at the forefront of surgical techniques and patient care standards. His holistic approach not only addresses cosmetic concerns but also enhances overall nasal function, leading to improved quality of life for his patients.
